Description
[UoA exercise science project] I investigated whether performing joint mobilisation tasks increased the risk of work-related musculoskeletal disorders (WMSDs) for physiotherapists. I analysed motion capture data using existing software to find RULA and REBA scores, low back compression forces, and joint strength capabilities at the most awkward posture for each task and subject. I then used R to perform two-way mixed ANOVA for each dependent variable. I found that all three tasks investigated can increase the risk of WMSDs for male and female physiotherapists.
Inspiration
Patient care activities such as lifting and transferring patients and the performance of manual therapy tasks such as joint mobilisation are likely to increase exposure to risk factors for work-related musculoskeletal disorders (WMSDs). Each activity involves the application of relatively high levels of force and or performance in awkward postures.
Joint mobilisation tasks are a type of manual therapy used to increase muscle function and reduce joint pain. The three joint mobilisation tasks investigated in this project are shoulder mobilisation, hip mobilisation, and pelvic joint mobilisation. These were selected from field observation and interviews with clinical therapists to find the most common tasks sustained for the longest time or the tasks with the most awkward body postures.
Process
To overcome the subjectivity of self-report methods, this project used an objective method of collecting motion data from three joint mobilisation tasks performed by physical therapy students. I received the motion capture data and ergonomic analysis results and performed the biomechanical and statistical analysis.
The analyses were carried out using an automated WMSDs postural assessment system. For ergonomic analysis, RULA and REBA scores were calculated at every time frame from the joint angle data. For biomechanical analysis, the low back compression force and strength capability of the body joints were calculated from the segment position data.
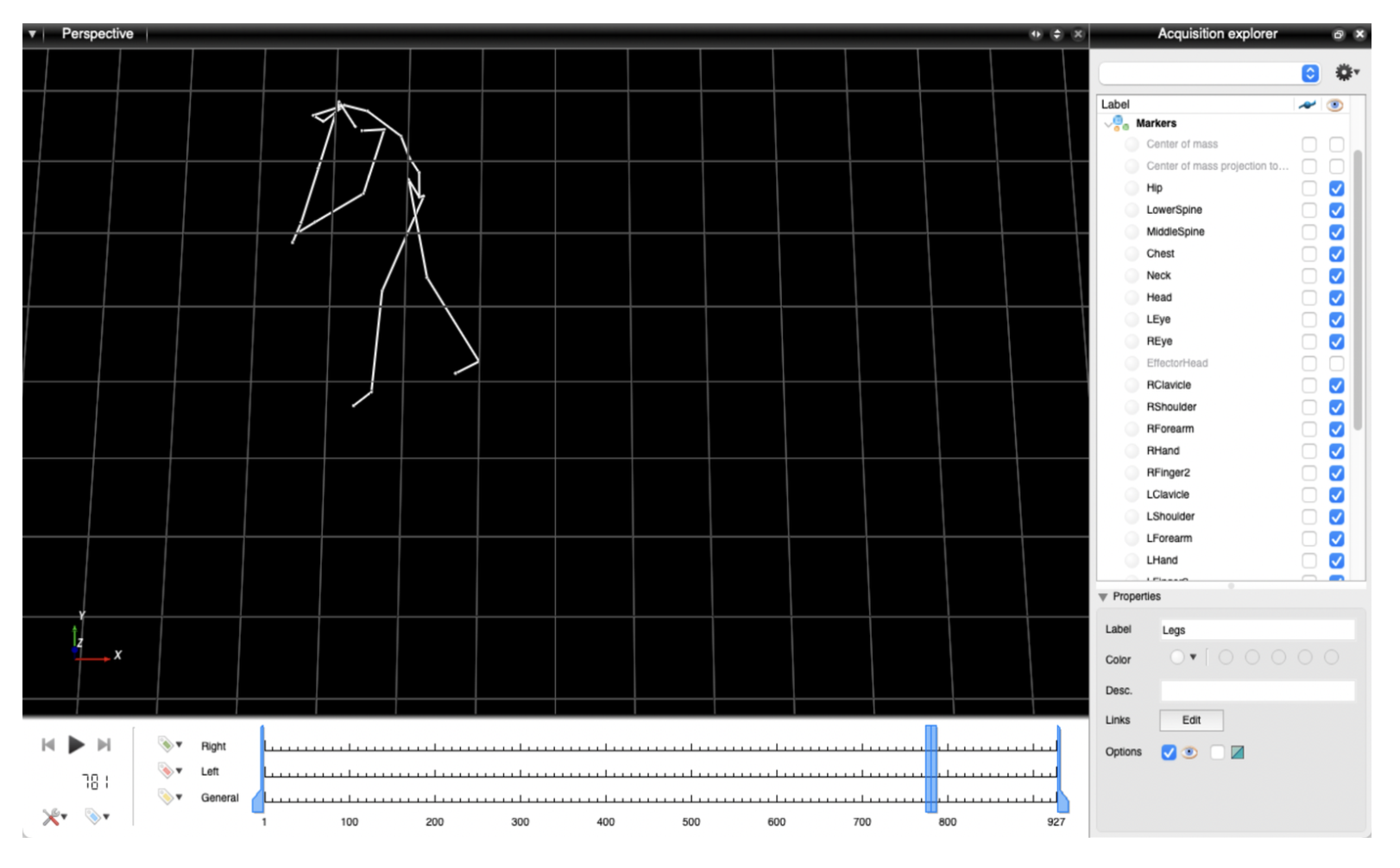
The motion data was visualised to identify the time frame of the most awkward posture for each task for each subject, defined as when there was the greatest flexion of the trunk. The corresponding results were tabulated to perform a two-way mixed ANOVA using R.
Learnings
All three joint mobilisation tasks investigated can increase the risk of WMSDs for both female and male physical therapists. This increased risk is likely to be caused by the performance of the tasks in awkward postures, particularly in the trunk and upper arms, rather than the application of relatively high levels of force. Future work could involve further investigating the effect of joint mobilisation tasks on the hands and wrists using more suitable data collection and analysis methods, and implementing changes to the tasks to decrease WMSD risk for physical therapists performing joint mobilisation tasks and conducting a follow-up study to investigate whether the changes were effective.